Outlive: The Science and Art of Longevity
Introduction
The author gave up medicine when he realized as a cancer specialist that he was only delaying the inevitable rather than curing them. But later he realized that we can actually put a stop to the source, i.e., our lifestyle, which mostly is the cause of the diseases we get.
1. Long game, from fast death to slow death
Longevity is not just how long we live but also the quality with which we live.
Most of the time, when we are admitted to hospital for a chronic disease, it’s too late and at the point where little could be done. The only good way is to change the source, the lifestyle. For example, the major reduction in people stopping smoking over the last decade has eliminated so many problems.
Emotional health is also very important, as it alone can decimate whatever things we have been maintaining physically.
2. Rethinking medicine for the age of chronic disease
The author says resistance to change and innovation at his place for usual medical procedures, made him want to quit.
It’s about the risk and reward factor, risk is more readily taken in other professions like banking finance but in Medicine, it’s more emotional than analytical emphasis is put.
There was an age old saying which got morphed to - Do no harm, which became the motto for surgeons. This doesn’t really make sense, coming from the old times, because they would follow more harmful procedures like bloodletting, drilling holes into skulls for headache, using mercury, which is super toxic, etc.
It is not saying that we should look for riskiest but short-term harm might not mean long term harm.
One example shared from author experience, was a patient who would have died in the elevator ride to operation room where the surgery could have been done in a sterile fashion. But there was a very high chance that he would have died if kept that long, so author had to operate him in the elevator itself, which did pose a huge risk but then again saved him. Sometimes doing nothing is the riskiest choice. Risk should be not straight up avoided but rather to be analyzed to work with.
Most chronic diseases cure isn’t readily solvable like cancer, etc. and they are in the body for a long time before they trigger and is too late to be saved most of the times.
Advancement to technology is also playing an important role in diagnosis and prevention of many diseases. Lot of gadgets which help patients to monitor their body health markers. Even when we go for tests, most are static which tell average data. For example, blood glucose is calculated when we fast and do tests to get an average value for the last 90 days. There are better ways now such as, use of devices which monitor blood glucose levels in real time, helping with much better diagnosis, taking a feedback driven approach.
Most medicine procedures, diagnosis etc. right now are on data which is taking average on a huge set of people, and applying the medicine based on that. The new technological advances are helping view each patient as a unique individual and not just treating everybody as the same.
We should start focusing on our quality of life (health span) for helping against diseases. Most medicine classes don’t really talk about things like how to maintain our physical and cognitive skills as we age, etc. - like exercise, having enough sleep, nutritional benefits.
3. Objective, strategy, tactics
Strategy is the overall plan while tactics is what we do to implement the smaller tasks at hand to achieve the result - the objective.
Post age 50, we usually see deterioration in physical and cognitive skills. We should try to plan now itself if we want to tackle how we live in the later years. We can follow the activities of daily living, which has basic things like walking unassisted, bathing and grooming, preparing meals, etc. Pretty simple when we are young, but gets harder as we age in our later years.
There is also emotional deterioration which can happen in young people too, something independent of age.
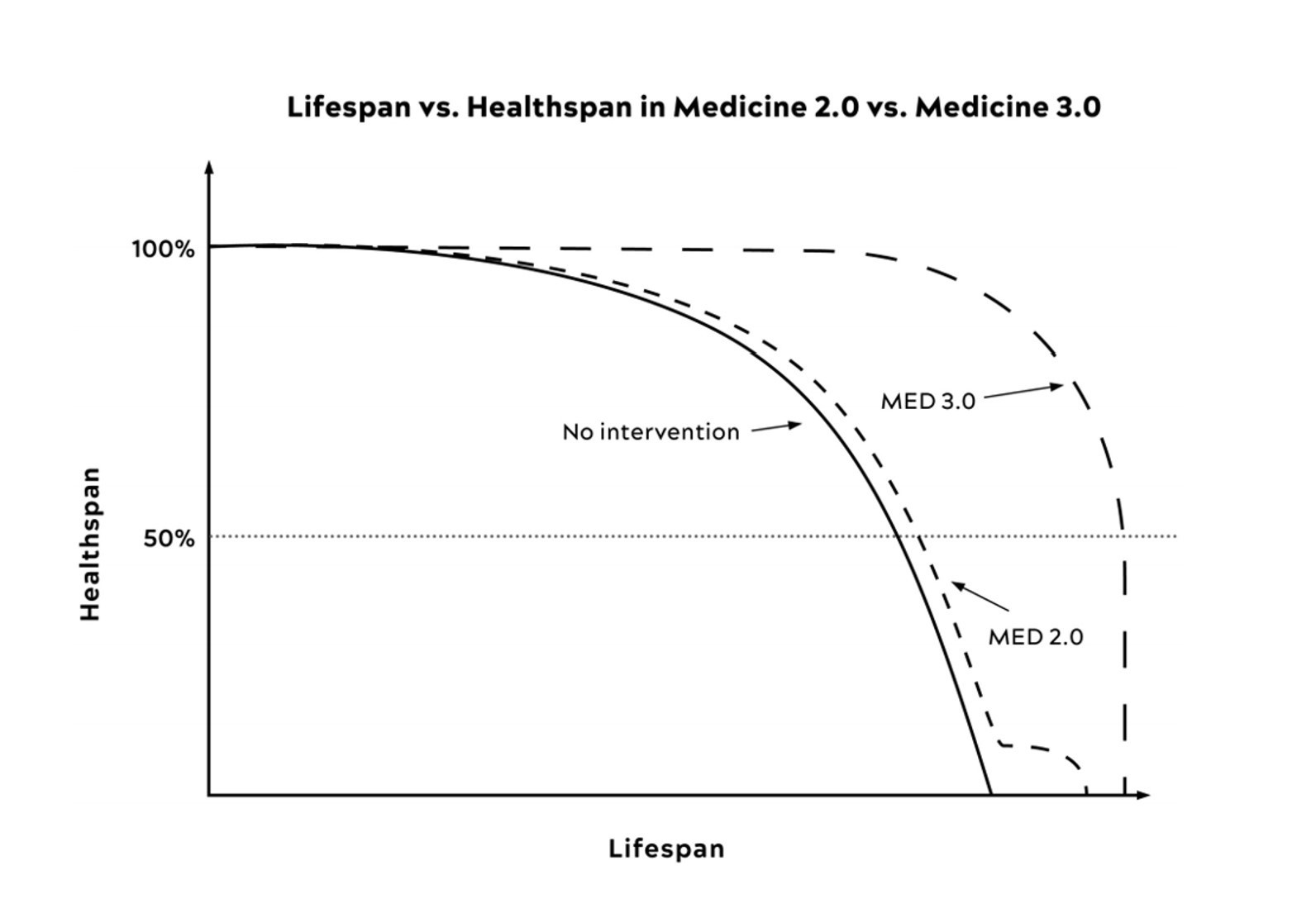
Med2.0 is the old medicine way where we treat the symptoms, but Med 3.0 preaches to change lifestyle, tackle the source.
Med 3.0 primarily asks to do these to help with healthspan,
- Exercise
- Nutrition
- Emotional health
- Sleep
- Exogenous molecules (like hormones, Supplements)
Exercise alone can help fight against so many ailments, especially cardiovascular exercises.
Sleep is also very essential, it helps retain our cognitive skills much longer, fight against mental health issues
4. Centenarians, the older we get the healthier we have been
Lot of centenarians have peculiar habits like drinking, smoking and aren’t really that health conscious as an average person. It is very likely that the genes are in play for their longevity.
What we can do is follow certain behaviors to get what the centenarians get for free via their genes, as getting their genes is out of picture.
Natural selection prefers traits which help us reproduce early in life not those which help us stay healthy for long, this explains why most people still carry genes like male patterned baldness, etc. this concept is called antagonistic pleiotropy, where a gene may have beneficial effect early on (boosting fertility, bond strength, etc) but harmful effects later (cancer risk, neurodegeneration). Hence, the bad genes are carried forward as natural selection doesn’t care to eliminate them.
So, to address these genes, we need to take extra measure by strengthening our cognitive skills, exercises, etc (the 5 things discussed in earlier chapters)
We should focus on delaying the onset of diseases instead of delaying the duration of the disease.
Another thing to note is that the research for tackling diseases are being done one at a time, that is separate research for cancer, for Alzheimer’s, for heart stroke, instead of finding the commonalities and trying to address those.
5. Eat less live longer, science of hunger and health
A molecule by the name Rapamycin, revolutionized the study of medicine, especially for transplant medicine. It was known to extend the maximum lifespan of people.
It was initially used for its antifungal properties but was later discovered to have immunosuppressive (suppress immune system - organ transplant, new organs are not rejected by immune system) and anti-proliferative properties (stops cells from multiplying - cancer treatment).
Researchers discovered that Rapamycin worked by inhibiting a protein complex inside cells that regulates growth and metabolism. This was named mTOR (mechanistic Target of Rapamycin) after the drug itself.
mTOR is present from yeast all the way to humans. As it is present in most life forms, it’s a very essential molecule according to evolution.
When we have enough nutrients, mTOR is activated which is responsible for cell division and going into reproduction mode, while when nutrients are scarce, it’s inhibited thereby the cells go into cleanup mode, stopping cell divisions.
It was the first molecule to increase longevity in mammals, and to give consistent results.
There is correlation on less food intake to longevity too. But that was made when doing for smaller animals like rats and might not be relevant to complex being like humans.
But in any case, if more nutrients were there the mitochondria would get oxidized over time or if not in use (being lazy I guess?) they would become less functional. When we do more exercise and have less nutrients than overdosing them, it helps in producing new mitochondria to replace them.
In specific, less amino acids seems to shut down mTOR and hence start the cell cleanup process to destroy old proteins and old cells into proteins.
But again, for a long time, given all these data points on rapamycin being a key driver to increasing longevity, we don’t use it on healthy people because of its immuno-suppressive effect. Then again, a derivative of rapamycin was found to have immuno-modulator effect - helps boost the vaccine effect. This suggested that rapamycin might not have immuno-suppressive but immuno-modulator.
It was then noted that it showed immuno-suppressive effect when taking low doses at intermittent times, while it showed immune modulator effect when taking medium to high doses with rest periods in between.
This is because there are actually two mTOR, mTOR1 and mTOR2. When taking daily both the molecules were inhibited but when taking it only briefly. Just mTOR1 was inhibited, which was seen to be the main molecule for longevity. Trials are happening around these findings currently.
People are more skeptical about taking these medicines – why take Rapamycin when we are already healthy? as medicines are usually taken when sick. That’s why the author is trying to show why med 3.0 is important to bring the shift in mindset.
6. The crisis of Abundance
Liver is body true workhorse. A healthy liver is normally in a deep dark purple colour with smooth texture. It seems most people have non-alcoholic fatty liver disease where fat builds up in liver without alcohol consumption. Liver is also known to regenerate a lot, donor and recover of liver transplant both recover fairly quickly.
Average is not necessarily optimal anymore. As the populace as a whole starts going overweight or showing symptoms of fatty liver, the average values of tests also skew over that direction. But those needn’t be optimal too.
Obesity used to be a main symptom if it would develop towards one of the horsemen, but author talks about Metabolic dysfunction, to be the more proper term, where you don’t always have to be obese for falling under the bigger set of problems like cardiovascular disease etc. These 5 criteria help see if we have it, (if you have any 3 of these at least then you have it)
- High Blood Pressure
- High triglyceride (type of fat which is stored in body when having excess calories)
- Low HDL cholesterol (this is good cholesterol which helps transports fat from bloodstream into liver for disposal, having less means more chances of buildup in arteries etc)
- Abdominal Obesity (waist length)
- Elevated fasting glucose
Metabolic health decides what happens to the calories we take, having metabolic syndrome means these nutrients go to places where they are not needed.
Insulin – hormones decide what to do with incoming calories for storing energy. Broadly it ends up in either bloodstream for quick use of energy or stored as fat. Fat cells are important as they help store excess energy. If it’s all in bloodstream it’s basically like us having diabetes; high blood glucose is harmful for kidneys, blood vessels, nerves, eyes etc. And if fat cells are full then the excess calories have to go into bloodstream which is bad.
Visceral fat or abdominal obesity on other hand is bad to have, as these fat cells are around the organs unlike subcutaneous fat cells in general which are spread throughout like arms, thoughts etc.
Visceral fat cells release chemicals which increase insulin resistance.
Once we have too much fat, it starts to spill into the muscles from around. Insulin resistant basically means that the cells (initially the muscle cells) stopped listening to the insulin signals. Imagine blowing a balloon, it gets harder to blow as it gets bigger. But there’s a limit to this, post which it just can’t hold any more air.
Cortisol hormone, which is associated with stress and sleep, is a double-edged sword which removed subcutaneous fat but replaced it with more harmful visceral fat.
Insulin-resistance also, is associated with cancer according to some studies.
Fructose in large quantities also showed an increase in insulin, elevated blood pressure and fat gain. The same molecule is available in almost all fruits etc. It also produces a lot of uric acid when metabolizing, which has negative effects. Most mammals which eat a lot of fruits have an enzyme Uricase which helps clear out uric acid, but this isn’t present in humans.
There were some studies on why we might have lost this enzyme, which attributed it to the evolution of humans. When apes were in Africa, there were abundant fruits to eat but when they migrated to Europe, where there was scarcity of food during winters, evolution went towards storing the extra energy in our cells. As a side effect they also lost the Uricase enzyme, Then these apes migrated back with their uricase silencing genes, and these eventually evolved into humans. Increased uric acid seems to increase lipogenesis (fat creation).
This is useless in modern times as we have a lot of food abundance and preservative methods.
But again, it’s very difficult to gain fat eating a lot of apples compared to table sugar because apple’s fructose is slowly digested with its fiber etc. Its not just fructose, but even a lot of preservatives give increased uric acid. So that’s why having a lot of fruit juice or foods with excessive preservatives are also bad.
When cells metabolize, they spend some energy to metabolize and then after metabolizing the food they generate more ATPs. There is an enzyme which controls how much energy a cell can spend for metabolizing, but for fructose case another enzyme does it, which doesn’t put any limits. So, the body thinks that energy levels are dropping too much when metabolizing when in-fact a lot of energy is going to be generated.
One test to check signs of early insulin resistance is, on empty stomach have a solution with high sugar (Doctors have this 75% sugar solution). If blood glucose levels remain elevated in the first hour, then insulin isn’t working at optimal rate. Ideally insulin should make sure it steadily goes into your cells.
7. Confronting and preventing heart disease
Calcium test via CT scan on heart arteries checks for calcification in arteries. At an early age we should have 0, but many don’t; Even though on the outside they look perfectly normal. Because most people have non alarming or an average score (given average is shifted because population as a whole is getting unhealthy), doctors as per MED 2.0 tell us it’s all good. But infact, it’s a sign to take care of ourselves.
Cholesterol is important to our body, and used to produce cell membrane, hormones etc. All cells produce it, but liver produces the most and ships it to others and retrieves it. It is not water soluble, so it cannot be dissolved in our plasma to transport it everywhere else. Instead they are transported as tiny sphericals called lipo-proteins (The L in HDL and LDL - which are part lipids(fats) (inside the structure) and part proteins (outside the structure)).
They are called LDL (low-density lipoprotein) and HDL (high-density lipoprotein) because of the ratio of fat (lipid) to protein they contain. LDL carry more lipids while HDL carry less lipids, as lipids are of lower density. There are also VLDL (very low density Lipoprotein) which are even harmful. Basically, HDL outer later has protein Apolipoprotein-A, while LDL, VLDL and IDL(intermediate density) ones have Apolipoprotein-B which seems to be present in the calcification signature/Atherosclerosis.
The cholesterol we eat such as from egg yolks etc, is just excreted and does little to contribute to Atherosclerosis. The vast majority of cholesterol in our body is actually produced by our own cells. Hence, we don’t really need to bother about over consumption of cholesterol food items. What is more problematic is the saturated fats consumed.
The Artery walls are actually permeable (the tissue area) and the LDL, HDL molecules can pass through it - in and out. But the LDL molecules (specifically, Apo-B part of it) stick to it. So it’s not cholesterol which is bad but the particles carrying it. Eventually the particles which are stuck are oxidised. Same is the case with VLDL and IDL, or anything with Apo-B. If too much of the oxidised cells are present, monocytes (large white blood cells) come, and become macrophages and try to eat up the oxidized cells. But if it consumes too much cholesterol, it blows up into foam cells. All of these line up to form some clump of fatty cells.
Here when HDLs comes across these foam cells, it would suck up the cholesterol using a process called delipidation. It also acts as an anti-oxidant for the artery cells. Though HDL helps us, increasing it via specialised drugs did not seem to give much benefit after some point, it’s more about increasing it’s functionality than the volume of it - for which research is currently going on.
This is still an active area of research — understanding what exactly drives antioxidant protection or helps clear oxidized cells. Interestingly, some patients and centenarians have been found to have very high LDL levels yet show no signs of atherosclerosis. However, in most people, atherosclerosis and arterial plaque development are very hard to detect in the early stages.
A CT angiogram (CTA) can help identify both calcified and non-calcified (soft) plaque, but it exposes you to more radiation than a regular CT scan. The author claims that in many cases, the information gained can justify the small added risk.
Over time, soft plaque becomes calcified, which is what shows up on a coronary calcium CT scan. However, the presence of calcified plaque also implies that there are likely other non-calcified (and potentially more dangerous) plaques that are not yet visible on the scan.
The author also said that the calcified plaque is stable while the non calcified (soft) plaque can rupture, causing a clot and thereby a heart attack due to the block in the passage.
The tests these days count number of Apo-B particles instead of LDL and HDL, as they are more meaningful, but most doctors still follow the old procedures.
Another deadly particle is the LP-a particle (Lipoprotein(a)), which is basically LDL with apolipoprotein(a). Due to the shape of it, it sweeps along any oxidised lipids along the way, so it kind of also helps clear out the passageway. But because it’s from the Apo-b family, it can also attach to the artery walls. And because of its structure it’s more likely to get stuck than LDL particles, along with the extra cargo of oxidised lipids, becoming more dangerous than LDL particles. More chances of causing plaques and ore mature heart attack.
We can only do limited things in reducing lpa(a) concentration but we can reduce Apo-B overall concentration, thereby reducing overall risk. But we can’t really lower them much with drugs without much side effects. There were also studies done where they tried to reduce HDL-C and increase, both didn’t give much benefit.
Smoking and blood pressure also damage the artery walls, thereby making it more easy for ApoB and other particles to get stuck
Saturated fat seems to increase synthesis of total cholesterol levels in body, and Apo-B particles. The excess saturated fat also seems to block the LDL receptors in liver thereby reducing the amount of LDL removed from circulation.
8. Cancer
The median age of cancer diagnosis is 66. The older we get the more prevalent the chances of cancer become. The cure for cancer is still far away, what doctors can do is to try and delay remission. In some rare cases a person’s immune system has fought and cured cancer.
Once a person gets cancer, there is a chance to get metastatic tumour (secondary tumour) - where the tumour cells move away from the primary site and start growing at other organs/tissues. This process is called metastasis. One example is breast cancer, metastasizing into the lungs.
It is this that is responsible for most cancer deaths. Even after removing cancer from the primary tumour, we never know if it has already spread elsewhere and is just waiting to gain a foothold there - it won’t turn up on any scans. That’s why people die when they get breast or prostate cancer while we do know that people can survive without these organs.
Cancer prevention is tricky as we don’t know the exact details yet unlike atherosclerosis and other diseases. Immunotherapy seems to show promise. Most importantly, it is crucial to find the cancer cells as early as possible, as it’s easier to deal with them at early stages.
People have tumour suppressor genes, such as PTEN, which regulate cell growth and prevent cells from forming tumours. In cancer patients, these genes are often found to be mutated or lost, which causes them to lose their normal function.
Research shows that there is no - one or common set of genes causing cancer, but random set of mutations which come together to evolve into cancer. Two women having breast cancer can have two completely different cancer genomes and they would need different cure for their cases.
Chemotherapy affects those cells more, which rapidly divide - the cancer cells. But this is also true for non cancer cells like hair follicles, gut cells, mouth lining etc, and hence the most commonly seen side effects are on these sites. But on the other side, if the cancer cells survive these procedures they become even more resistant.
Compared to normal cells, many cancer cells have altered metabolism, consuming huge amounts of glucose. They also have some uncanny ability to evade the immune system cells. If we were to solve these, we may get to target cancer cells only and sparing the non cancer cells, thereby the patient.
Coming to the metabolic part, most healthy cells use aerobic respiration which produces around 36-38 ATP cells but cancer cells use anaerobic respiration (don’t use O2) and give only 2 ATP cells. This is called the Warburg effect. We can use these findings to find cancer cell spots in the body, a radioactive high concentration of glucose is sent to the body and a pet scan shows where are the places with high glucose levels.
But they do produce a lot of byproducts when doing anaerobic glycolysis which are used as building blocks for new cells. Another finding is that, the lactic acid etc produced as by products reduce the pH and the immune cells can’t function as good as normal.
One key connection among obesity, smoking, and insulin resistance is that they all promote chronic inflammation, which in turn creates a biological environment that increases the risk for many chronic diseases, including cancer.
Elevated insulin levels can act as a cancer enabler, because insulin — along with insulin-like growth factor 1 (IGF-1) — activates growth-promoting pathways (such as PI3K–AKT–mTOR). These pathways stimulate cell growth and proliferation while increasing glucose uptake by cells. When chronically elevated, this signaling can fuel tumor cells, which thrive on glucose and rapid growth.
There was a study about using drugs to reduce PI3K to tackle breast cancer. Only one person survived it, in that study, but one differentiating factor was that she strictly had low glucose diet. It was later noticed that, reducing PI3K would mean cell pathways to let glucose into cells was blocked, which meant more glucose staying behind in the bloodstream, which in turn meant more insulin production , which defeats the purpose - having low glucose diet like ketogenic diet, definitely helped.
In Outlive, Peter Attia explains that T cells (T lymphocytes) are the immune system’s “assassins” designed to detect and destroy abnormal or cancerous cells. However, cancers often evade them by exploiting immune checkpoints that switch T cells off. The development of checkpoint inhibitor therapies—drugs that release these immune brakes—has allowed T cells to once again recognize and kill cancer cells, leading to remarkable cures in some cases.
As cancer grows there simply aren’t enough T cells to detect and kill them. Adoptive Cell Transfer (ACT) - sometimes referred to as CAR-T cell therapy - where doctors take a patient’s own T cells, modify or multiply them in a lab, and then re-infuse them into the body to hunt down and destroy cancer cells. These engineered T cells can be designed to recognize specific tumor markers that normal T cells might miss.
These can be genetically modified or some isolated tumour cells can be taken and checked with body’s T cells if specifically any of them are able to kill them, and then those are multiplied and reinfused.
Our early stage cancer discovery systems are also not there yet. Lot of false positives and false negatives are present. With multiple tests, we get more clarity.
- Sensitivity measures how good a test is at detecting disease when it’s truly there — in other words, its ability to catch true positives. A highly sensitive test minimizes false negatives, meaning it’s unlikely to miss a case of cancer.
- Specificity, on the other hand, measures how good a test is at correctly identifying people who don’t have the disease. A highly specific test minimizes false positives, meaning it won’t mistakenly flag healthy people as having cancer.
9. Alzheimer’s Disease
Apo-E correlates to Alzheimer’s, which is responsible for lipo transport and metabolism in brain. It gas three variants - E2, E3 and E4.
Everyone inherits one copy from each parent, so you can be:
- E3/E3 (most common, “neutral” risk)
- E2/E3 or E2/E2 (slightly protective)
- E3/E4 or E4/E4 (higher Alzheimer’s risk)
These and other neuro-degenerative diseases don’t have any cure yet but we can try our best to prevent them:
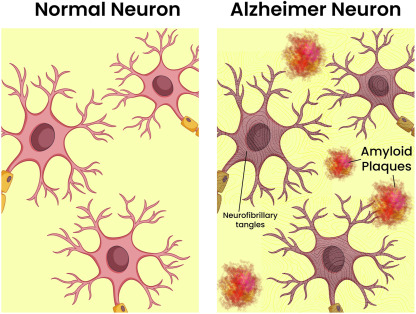
- Alzheimer’s: Memory-loss dementia caused by buildup of amyloid and tau proteins that damage brain cells.
- Lewy Body Dementia: Dementia caused by alpha-synuclein (Lewy bodies); leads to hallucinations, alertness changes, and movement problems.
- Parkinson’s Disease: Movement disorder from loss of dopamine neurons; later can cause dementia due to Lewy body buildup. Also affected by alpha-synuclein.
There are E4/E4 centenarians too, who likely have other genes who protect them from Alzheimer’s. So just having E4 doesn’t guarantee a diagnosis of Alzheimer’s.
The brain makes amyloid precursor protein (APP), which helps with neuron growth and repair. Normally, enzymes cut APP into harmless fragments. But when it’s cut the wrong way, it produces amyloid-beta, a sticky protein. These fragments clump together to form plaques between brain cells, disrupting communication and triggering inflammation. Over time, this leads to neuron death and Alzheimer’s disease.
Tau helps stabilize the tiny structures (called microtubules) that transport nutrients and signals within brain cells.
Basically,
Amyloid-beta builds up outside neurons (plaques).
Tau tangles form inside neurons, causing inflammation and brain shrinkage.
Together, they drive the brain damage seen in Alzheimer’s disease.
Currently, this is the dominant theory right now and not conclusive that it by itself is the reason for Alzheimer’s. There were drugs developed to stop or reduce the Amyloid-beta production but the benefit is yet to be seen on the patients, but again these were tried on patients who were already on late stage - as they were identified later.
There are many studies which question the correlation with Amyloid-beta and there are also lot of dementia patients with little to no build up of amyloid-beta; making it seem like it’s neither a sufficient or required condition for Alzheimer’s.
Subtle brain changes begin long before the early, diagnosable stages of Alzheimer’s disease. These changes can occur years or even decades before memory loss becomes noticeable. Standard cognitive tests, such as recalling a list of words or repeating phrases, often fail to detect this early decline because they measure only obvious symptoms that appear later. By the time such tests show impairment, significant damage may already have occurred in the brain.
Doing cognitive exercises clearly helped delay the Alzheimer’s process. Same is true with movement exercises for Parkinson’s disease. More complex the better, for example, dancing is better at delaying the progress than walking.
Some tests on rats show that restricting blood flow in brain, was also causing memory related issues and them being more severe in old ones. Even for us, as we age it’s possible for atherosclerosis to occur in the brain blood vessels. These studies also tried to show that amyloid-beta and the tangling is more of a product than the cause.
Having Diabetes increasing the chance of Alzheimer’s, as:
With diabetes/insulin-resistance, your body’s ability to handle glucose is impaired, meaning higher circulating glucose, higher insulin, more variability, etc.
- This metabolic dysfunction damages blood vessels (including those in the brain) and leads to poorer perfusion (blood circulation).
- At the same time, neurons may struggle to use glucose effectively (or insulin signalling in the brain may be impaired) so their “fuel” supply is compromised (more on this below).
- The hippocampus and other brain areas critical for memory are especially vulnerable to metabolic dysfunction, so the damage accumulates.
- Genetic vulnerabilities (like APO-E E4) may worsen how metabolic dysfunction affects the brain.
- Over time, this combination facilitates the pathological changes seen in Alzheimer’s (neuron loss, dysfunction, accumulation of amyloid/tau, etc).
Why are insulin receptors in brain if brain doesn’t store any energy?
Insulin in fat or muscle says “store energy”, but in the brain it says “maintain synapses, protect neurons, and coordinate metabolic signaling.”
Studies also showed that E4 is poorer than the other variants in moving cholesterol in and out of the brain.
Evolution wise the original ancestors have E4/E4 variants and were largely helpful against infectious diseases, the inflammation in brain helped fight these off but they are harmful in our modern life.
Exercise, especially endurance, helps the mitochondrial functionality and strength training. Specifically grip training seems to help Dementia cases. Apparently, sauna and maintaining oral health also helps.
10. Framework of Principles
Things we could do to tackle all the chronic diseases we have seen before:
- Exercises - aerobic and strength both
- Diet and nutrition
- Sleep
- Techniques and tools to improve emotional health
- drugs, supplements and hormones, basically the Exogenous molecules
11. Exercise
Both cardio and strength training are equally important. But compared to doing nothing, even walking is good.
One important biological marker is peak aerobic cardio respiratory fitness using VO2 - the max rate at which a person can utilize oxygen.
On the other hand, just big muscles aren’t enough, those muscles should be able to create force.
Exercise also helps with brain health - it releases molecules which improves memory, and also signals body for better bone and immune system.
Excelling at one sport is good, but lets say going all in on cycling only helps your lower body. Thats why the author emphasised that we should also be generic enough, and be able to do wide variety of things.
12. Stability
Stability is very important while doing exercises, be it cardio or strength training. It’s about us not getting injured while doing them.
Glucose can be converted to energy in multiple ways but Fats can be converted to energy only in the Mitochondria. Typically, lower intensity workout burn fat while higher intensity workouts burn the glucose.
Exercises can be split into zones. Zone 1 being normal walk, Zone 5/6 being sprinting with us going all in. Zone 2 is recommended for fat burn.
Athletes can easily switch between the fuel sources - fats/glucose. Usually for low intensity workouts or movements, fats are preferred for fuel, but in the case of sedentary people - they are stuck with glucose consumption even for simple things. The fats are just stuck in the cells, making it very hard to lose fat.
Lactate is produced during glucose consumption when your cells run low on oxygen or when the energy demand is so high that the oxygen-based pathway can’t keep up.Lactate monitor helps check how much lactate is being produced. It by itself is not harmful, but paired with hydrogen ion it becomes lactic acid, which causes pain and stiffness in muscles. Body can cycle the lactate but it also depends on - how much can it recycle. Anything more than your current limit, lactic acid is produced.
Zone 2 produces ~2 milli-moles/L of lactate. Primarily, fat is burned but glucose use is also present. This zone is where we can hold conversations but it is a little bit strained, going to any higher zone means that it’s hard to hold conversations.
If our goal is to raise VO2 max - maximum rate at which your body can take in, transport, and use oxygen during intense exercise; then we need to concentrate more on zones which make us reach there - higher zones.
We use type 1 muscle fibre for doing daily things but unless we push ourselves with heavier weights, the type 2 muscle fibres would wither away, causing loss in muscle mass and strength.
This process fastens up if we are sedentary and just eat excess calories. This is because one of the main destination of fat spillover is muscles.
It is important to note that it is very difficult to get more muscle mass as we age.
Body fat percentage and Bone mineral density are also essential markers to check. As we age, BMD decreases and lose muscle mass, especially when we don’t have enough nutrition. BMD and Muscle mass helps us with stability.
Carrying things is a great way to do exercise. One can look at Rucking, which is walking or hiking with weighted backpack.
Grip strength exercises are also very important, such as farmers carry, dead hangs, etc.
We should take consideration of all angles when doing exercises so that all muscles are involved.
Hip hinging movements are important too - basically legs, glutes and lower back.
We need to train and check on following too:
- Concentric strength is when muscles shorten to create movement, like lifting a weight or standing up from a chair. It builds power for everyday actions.
- Eccentric strength is when muscles lengthen under tension, like lowering yourself into a chair or walking downstairs. It improves control and prevents falls.
- Isometric strength is when muscles hold steady without moving, like in a plank or holding a bag still. It builds stability and balance.
Chapter 13
Lot of people stop exercise after getting some injury. That’s why stability is very important and we need to take care so that we don’t get injured.
It’s not just imbalance, rigidness, it’s about how efficiently can we transmit force safely. If only some of the force generated is being utilized, the rest has to go somewhere. Typically, it choses the path of least resistance which is our joints, spine, etc.
Dynamic Neuromuscular Stability (DNS) — a concept from rehabilitation science that focuses on how the brain, muscles, and joints coordinate to maintain proper posture, balance, and movement control.
The idea is that movement quality, not just muscle size or endurance, is what keeps the body functional and prevents injury as we age.
The author emphasizes that this coordination begins in infancy, where we learn fundamental patterns like rolling, crawling, and standing. DNS training aims to retrain those natural patterns that often get lost due to poor posture, sitting habits, or overtraining specific muscles.
Breathing correctly is also important, be it weight training or for cardio. Stay flat on ground, place one of your hand on stomach and other on chest. When you inhale, check what hand rises up. Based on it we have three categories -
- The Hyperinflated Guy
- This person is always in a chest-up, rib-cage-flared position — like they’re perpetually taking a deep breath.
- Their diaphragm doesn’t descend properly, so their breathing relies heavily on the chest and neck muscles.
- This leads to tight lower backs, stiff necks, and limited mobility, even though they may look “fit” or”upright”.
- Many athletes or gym-goers fall into this category because they overtrain without focusing on proper breathing mechanics.
- The Sad Guy
- Characterized by a collapsed chest, rounded shoulders, and forward head posture.
- The diaphragm is again not functioning well — this time because the rib cage is compressed downward.
- This pattern restricts lung expansion, reduces oxygen efficiency, and contributes to low energy, back pain, and poor movement control.
- Common among people who sit for long periods or have sedentary lifestyles.
- The Yogini
- Represents extreme flexibility but poor stability.
- They can bend deeply but lack muscular control around their joints, leading to instability and potential injury.
- Flexibility without strength and coordination doesn’t equal healthy movement.
- The goal isn’t to be the yogini but to find balance between mobility, strength, and control.
One need not just belong to one but can overlap.
Feet also plays an important role. It controls posture and also dampens force before it reached knees, joints and back. We should take care about the kind of shoes we wear.
We also need to put our feet flat and not put weight only on outer edges(supinated) or inner edges(pronated).
Must do joint exercises - https://peterattiamd.com/outlive/videos/
14. Nutrition
Lot of people talk about a one diet being best - vegan, carnivore, vegetarian, ketogenic etc. There is no one best diet. We need to figure out based on what our body needs.
We need to check if we are
- over/under nutritioned
- adequate/under muscled
- Metabolically healthy
Most experiments require group of people to adhere to a strict diet to get findings which is hard to enforce, so most studies aren’t that definitive - cannot be trusted so much. Most studies have a healthy user bias where the baseline health of test group is inferred than the actual input. Maybe a part of the test subjects were very healthy so more tolerant towards a particular input, vice versa.
Chapter 15
Companies have a goal to get their products available for higher reach, better storage, easy transportation and more palatable; but they don’t have a criteria to make them harmless. Many foods have:
- Added sugar
- Highly refined carbohydrates with low fibre content
- Processed oils, dense caloric foods.
which is all basically junk food.
Most diets which people follow have atleast:
- caloric restriction; total intake in a day
- dietary restriction; eating less of particular elements like red meat, sugar etc
- time restriction; eating at specific times or fasting
Most people skip protein.
For caloric restriction, counting calories with apps is very helpful. Even in studies with monkeys, where a part of them were fed as much as they wanted and while the other part restricted. It was noted that benefits were much more obvious when they were using processed food than natural food.
For dietary choices, think about what food is calorically dense and try to single them out and restrict/avoid them. Usually restricting carbs help because there are very less choices for ketogenic food and they kind of make you more full than carb based diet. Still having processed fat/saturated fats aren’t good for health, so make note of that - lets say no carbs but unlimited beef, thats still bad. Even with dietary choices, let’s say you are vegan, you can still gain weight if you eat too much of anything.
Also same diet wont work for multiple people, what works is different for each person.
Alcohol is very caloric dense and has no nutritional benefits. It delays the fat oxidation. It also promotes mindless eating. It’s hard to restrict to moderate levels for which some studies showed benefits, anyway. The author suggests no more than 2 glasses per day and 7 glasses per week, if we must have.
Continuous Glucose Monitor (CGM) is a good device which helps us find trends on how our body behaves on our diet. For some people some foods give spikes in CGM while some don’t.
The more refined the carbs, the higher the spike. If they have any fibre content, it helps blunt the spike. White rice and oatmeal also give spikes as they have high glycemic index.
It’s normal for glucose to spike while exercising, especially strength training, as the liver sends more glucose for energy consumption.
A good / bad sleep affects heavily on the spike levels.
Unsaturated fats, leafy vegetables have no effect on blood glucose. But large amounts of them have a small rise though.
Most important benefit is, because we are tracking or observing, we tend to be more conscious of our choices.
Unlike fats and carbs, protein isn’t stored for energy. Though it can be converted to glucose in the liver, that is not the primary source nor the preferred way for consumption.
Excess is usually excreted via urine.
They are used in muscles, hair, skin and even help forming antibodies in our immune system.
There are studies on mice, or general guidelines that low protein diet like 0.8g/kg might be beneficial but the author disagrees.
The author recommends 1.6g/kg for normal people and 2.2g/kg for active people with good kidneys. We shouldn’t have all of it at once too, as that would oxidize it and convert it to energy. Spreading it out in various meals is better. Since it is hard to achieve, a protein shake and snack is helpful to achieve this along with protein meals.
The thing about protein from plants is, it is tied up with the indigestible fibre and not largely bio-available for absorption. We could tackle this a bit by cooking, but there’s still an another issue. The distribution of amino acids is not the same as that available in animal protein, and have less essential amino acids - in particular, they often contain lower amounts of certain essential amino acids such as methionine, lysine and tryptophan, effecting the muscle protein synthesis.
The same is true when comparing whey protein isolate and soya protein isolate.
Protein also makes you feel satiated.
Fats are more calories but are still essential and they help with slow oxidation as fuel as well essential block for hormones and cell membrane. It is also required in the brain in the form of fatty acids.
Roles of different fats in longevity. - MUFAs (monounsaturated fats): Best for health. Found in olive oil, avocados, nuts. Improve heart health and insulin sensitivity. - PUFAs (polyunsaturated fats): Include omega-3s (good, anti-inflammatory) and omega-6s (can be harmful in excess). Get omega-3s from fish; avoid seed oils high in omega-6s. - SFAs (saturated fats): Found in butter, meat, dairy. Not automatically bad, but too much can raise LDL particle count. Monitor blood markers instead of avoiding all SFAs. Overall: Favor MUFAs, include omega-3 PUFAs, limit seed oils, and watch biomarkers rather than following strict fat rules.
The saturated fats are linear in structure and tightly packed, and hence tending to be solid at room temperature. The unsaturated fats have double bonds, kinks in their structure and are loosely packed, liquid at room temperature . They also react easily with other molecules compared to saturated fats. No food has one type of fats only though. Palm and coconut oils are very close to saturated fats while olive oil is very close to mono-saturated fats.
There is also trans-fats which have been banned. They prolong shelf life but are very harmful. Some food labels used to have them as partially hydrogenated vegetable oil.
While fasting has a lot of benefits - improves cellular regeneration, mTor is inhibited, reduces hunger (as fats are getting oxidized), the author doesn’t recommend this for everyone. The 8hr eating window and 16hr fasting window, became very popular but was actually tested in mice. For an animal with 2-3 yr life expectancy, 16hr window is like a multi day fasting for humans so its just isn’t a valid comparison. Hence, 16 hr is too less of a window to obtain all of the fasting benefits.
It’s also likely for one to skip their protein requirements and binge eat in their allowed window. Especially for lean people, long windows of fasting, would make you lose weight along with muscle mass which is bad.
Author concludes that if he could eliminate one type of food, it would be fructose sweetened food sources and fruit juices (as they lack fibre).
16. Sleep - the best medicine for brain
Sleep deprivation makes us do a lot of mistakes and makes it hard to concentrate. It increases metabolic dis-function, increases insulin resistance and hormonal imbalances. Our performance drops and it is more clear if we are athletes. We also look older and have flabbier skin.
Poor sleep also increases stress. It makes us feel irrationally hungry the next day, increases cortisol levels causing increased blood pressure.
Every animal sleeps in some way ( dolphins sleep using one half brain, horses sleep standing, etc) but evolution has not discarded sleep.
Many studies showed we need to have atleast 7.5-8.5 hrs of sleep. Even having too much sleep - 11hrs etc, is bad.
Sleep has different stages:
- Non-REM (NREM) sleep
- NREM sleep is divided into three stages (N1, N2, N3) after you fall asleep.
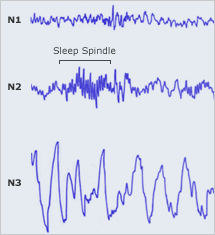
- Stage N1: The lightest sleep; moving from wakefulness into sleep, theta waves appear, easy to wake. ~5% of sleep time.
- Stage N2: “Light sleep” but deeper than N1. Characterised by sleep-spindles and K-complexes in EEG (Electroencephalogram, a test to study brain waves and sleep cycle). Makes up the largest portion of sleep (~45% for many adults).
- Stage N3: Also called “deep sleep”/”slow wave sleep (SWS)”. High amplitude, low frequency delta waves. Hard to wake from; restorative body functions are strong here. SWS - slow wave sleep, as brain’s electrical waves are large and slow.
- Deep NREM is when the brain clears out its cache of short-term memories in the hippocampus and selects the important ones for long-term storage in the cortex. Also, during deep sleep, the brain activates a “waste disposal” system (cerebrospinal fluid flooding between neurons, clearing inter-cellular junk including amyloid-beta and tau) which is linked to preventing neurodegenerative diseases like Alzheimer’s disease.
- NREM sleep is divided into three stages (N1, N2, N3) after you fall asleep.
- REM sleep
- REM = rapid eye movement sleep. Brain activity in many ways resembles wakefulness (desynchronized EEG), but the body is largely paralysed (muscle atonia).
- Dreams predominantly occur in REM. It’s also important for emotional processing, memory consolidation, and creative problem-solving.
- REM contributes to emotional regulation, creativity, procedural memory (skills), and forming neural connections — especially in younger brains.
The chapter emphasises sleep quality, not just quantity. If you get enough hours in bed but have fragmented sleep, reduced deep sleep or REM phases, you may miss the benefits
Some terms discussed:
- Sleep Spindles: Short bursts of rapid brain activity seen in N2. They help protect sleep and support memory consolidation.
- K-Complexes: Large, isolated brain waves during N2. They help keep you asleep despite external noise or stimuli.
- Delta Waves: Slow, high-amplitude brain waves seen in N3 (deep sleep). Reflect very synchronized, restorative brain activity.
- Muscle Atonia: A temporary paralysis of nearly all skeletal muscles during REM sleep. It prevents you from acting out your dreams.
- Desynchronized EEG: Brain waves during REM look irregular and fast — like when you’re awake — even though you’re asleep.
When we are sad before sleep, because it helps with emotional balance, we feel better the next day. We remember the event and not the emotional attachment. Its like PTSD, if we are unable to do this and highly correlated to the fact that the are unable to get into REM sleep. Having less REM sleep, also makes us hard to understand others facial expressions and emotions. Some studies showed others having neutral expression was seen to be menacing.
Poor-quality sleep is strongly correlated with Alzheimer’s disease. In fact, most Alzheimer’s patients show years of reduced or irregular sleep cycles before diagnosis, and the relationship appears to be bidirectional — poor sleep accelerates the buildup of toxic brain proteins, while those same changes further disrupt sleep. Cognitive health is also deeply intertwined.
Growth hormones are also released post an hour of getting into sleep, with the peak being for those in adolescence.
The sleep drugs in the market dont let you go to deep sleep, so they arent giving us quality sleep. It might help us tracking us sleep schedule and stages (apps do it based on breathing, heart rate etc) to optimise. But for people who have a hard time sleeping they get stressed out with the metrics so it’s probably better for them to not have. Dark rooms help sleep better. Darkness activated hormone, melatonin lets our brain know that it’s time to sleep. But LEDs, like phones, some lights doc are on the blue end of spectrum, resembling more of day light, which makes it harder for us to fall asleep. Keeping the bedroom cool also helps. Alcohol makes it harder to sleep for the later stages of sleep and makes it harder to sleep in the later half of the night if we wake up. Hot bath and sauna also helps. Try to stay on same sleep schedule even on weekends. Sone people are genetically wired to sleep late, so if others dont help we can try shifting our sleep schedule. If nothing above helps, there is cognitive behavioral therapy for insomnia (CBT-I).
Caffeine helps block sleep by blocking Adenosine receptors, where usually Adenosine gradually accumulates when we are active.
Caffeine has a half-life of approx six hours (meaning that if you consume a cup around noon, roughly half of it remains active by ~6 pm), but again depends on each person’s metabolism.
17. Emotional Health
Feeling lonely and having poor mental illness effects our longevity. This isn’t always about diagnosed mental illness but emotional distress plays a huge role and is harder to identify and treat.
Trauma is of five categories:
- Abuse: physical, sexual, emotional or spiritual
- Neglect
- Abandonment
- Enmeshment, blurring of boundaries between children and adults
- When a parent (or adult) relies on a child for emotional support, companionship, or validation, in ways that a child isn’t developmentally ready for. The roles get reversed — instead of the adult caring for the child, the child becomes the caretaker or emotional partner.
- witnessing tragic events
Children adapt in different ways for trauma, but the problem occurs when they grow up to be dysfunctional adults.
There are four patterns:
- Addiction (needn’t just be material abuse, can also be work, exercise,etc)
- co-dependency/excessive psychological reliance
needing others for validation and survival - Habituated survival strategies (anger and rage)
- attachment disorder (emotional detachment)
unable to trust or bond
The usual mental illness like schizophrenia have known symptoms but emotional distress are harder to treat and root cause.
A truly fulfilled and long life must align more with eulogy values than resume ones. Resume Values
- These are the things you put on your résumé — achievements, skills, status, success markers. e.g., “I’m a doctor”, “I built a company”, “I hit my fitness goals”, “I won awards.”
- They are external and focused on achievement, productivity, and image.
Eulogy Values
- These are the qualities people would talk about in your eulogy — who you were, not what you achieved. e.g., “He was kind, patient, generous, loving, loyal.”
- They represent character, relationships, and meaning - what kind of person you are to others and yourself.
When our lives are driven purely by resume values, we often achieve a lot - but remain emotionally empty, disconnected, or anxious. Shifting toward eulogy values helps create emotional stability, purpose, and connection, which are vital to psychological and even physical longevity.
Also we should not be very hard on ourselves. They help us mostly with resume values which don’t matter towards the end. Imagine if the same things you are bring hard on yourself are being done by your friend or family member, would you react the same?
Four pillars of emotional fitness that we need to be mindful to begin with:
- emotional regulation, control on emotions
- distress tolerance, ability to handle emotional stressors
- interpersonal effectiveness, how well we make needs and feeling known to others
- self management, taking care of ourselves, even basic things like getting up on time
When we’re hijacked by stress or anger, the sympathetic “fight-or-flight” system takes over. A simple reset—like splashing ice-cold water on the face or taking a cold shower, activates the parasympathetic response, calming the body so the mind can follow. Deep breaths also help.
It’s also good to take walks, try rucking without any distractions like phones.